Most professionals have tried to study the human response to intercourse activities, including Freud’s psychotherapy and Kinsey’s sexual orientation scale. Sexual disorders include all the issues that appear at any stage of the sexual response system and hinder the enjoyment of sexuality (Reed et al., 2016). These dysfunctions are brought about by physical discomfort during intercourse, incapability of having sexual intercourse or reduced want or need for intercourse. A discrepancy between a person’s physical gender and the gender they identify is known as gender identity disorder. People with gender identity disorders could experience extreme discomfort regarding their physical gender and development after puberty.
Definition of Sexual Disorder
The sexual disorder is an arousal pattern that lasts for some time and may cause stress and social challenges to the patient. According to the DSM-IV, the triphasic model of the sexual response pattern include desire, arousal, and orgasm. The four main categories of these disorders include disorders of desire, arousal, orgasmic experience, and pain. Physical causes of the sexual disorder include hormone issues, alcohol, and drug abuse, heart issues, and neurological disorders. Lack of interest in sex is a sign of desire problems. The inability to excite physically or sexually is an indication of arousal problems. Orgasm problems are characterized by orgasmic reticence or incapacity (Solis-Moreira, 2021). Lastly, pain during sexual activity is a sign of pain disorders.
Types of Sexual Disorders
- Desire Disorder
On the other hand, desire disorders are marked by a significant decrease in sexual interest. Individuals who experience these disorders had once higher levels of desire in their lives. However, the desire decreased due to psychological causes such as relationship issues, which affect the emotional connection needed for a majority to experience sexual desire. Physical issues such as hormone imbalance causing lowered testosterone levels in individuals with the male reproductive system and alterations during menopause for those with a female reproductive system may also lead to decreased sexual desire. Two categories related to desire dysfunction are female arousal disorder and male hypoactive sexual disorder (Avasthi, Grover, and Rao, 2017). Mental health and hormone therapy are among the best treatments for those suffering from this disorder due to psychological and physical issues.
- Arousal Disorder
The inability to react to either mental or physical sexual cues is a sign of arousal dysfunction. Mental responses include imagining sexual affairs, close intimate contact, and actual physical sexual stimulation. Individuals with the male reproductive system experience erectile dysfunction (ED), signalled by the incapability to hold an erection. Individuals with the female reproductive system with physical indications of an arousal disorder may have vaginal dryness or no genital sensation. Hence, a lack of mental and emotional stimuli resulting in a lack of physical response (Avasthi, Grover, and Rao, 2017). Treatment for arousal disorder may include medication prescribed by a doctor.
- Orgasmic Disorder
An individual unable to have an orgasm is said to have orgasmic dysfunction. It is referred to as female orgasmic disorder for individuals with a female reproductive system. The diagnosis for individuals with a male reproductive system is erectile dysfunction, premature or delayed ejaculation. Female orgasmic disorder falls into two categories: main and secondary. The female orgasmic primary disorder is where the female has never had an orgasm.
In contrast, the secondary female orgasmic disorder is where a female cannot achieve orgasm following a disturbing occurrence. In addition, physical ailments such as damage to blood vessels around the pelvic area can lead to orgasmic disorder. The most common psychological issue leading to orgasmic disorder is trauma or abuse.
- Pain Disorder
Pain disorders involve experiencing pain during intercourse. It comes in two types, dyspareunia and vaginismus. According to Reed et al. (2016), dyspareunia is persistent or repeated vaginal pain brought on by sexual activity. A reduction in arousal or sexual desire that results in dyspareunia causes pain. Some factors that reduce sexual desire include stress, tightened vaginal muscles, guilt related to sex, body insecurities, and relationship problems. It affects both men and women and may be caused by physical injury to the pelvic ligaments (Giorgi, 2020). A doctor can treat dyspareunia through medications.
- Vaginismus
Vaginismus, on the other hand, involves pain and involuntary contraction of the muscles around the vagina. The contractions make penetration difficult, including non-sexual penetration, such as tampon insertion. According to Tarrant (2022), it is an ongoing, unconscious spasm of the vaginal muscles that prevents sexual activity. Vaginismus is treatable through topical therapy; pelvic floor therapy, where a physical therapist teaches how to relax the pelvic floor muscles. Vaginal dilator therapy helps stretch the vagina. Cognitive behavioural therapy helps in mastering how thoughts affect emotions and sex therapy.
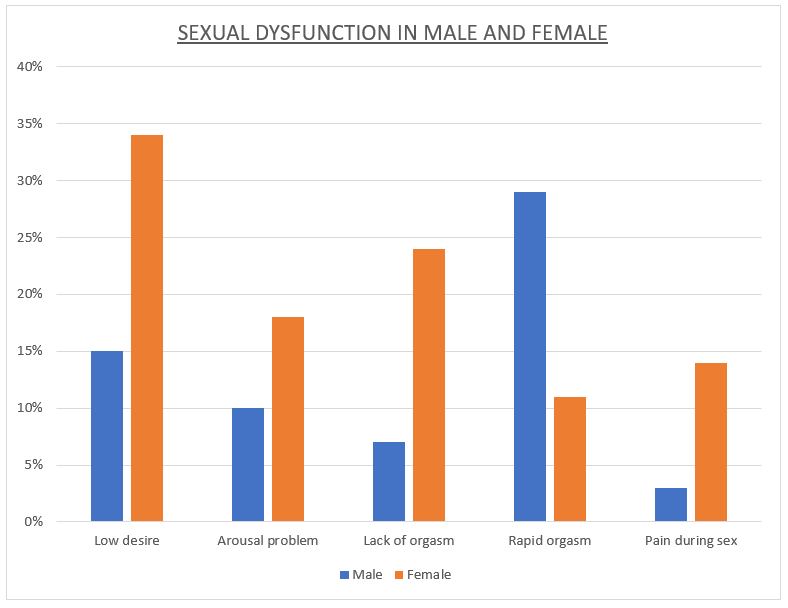
Figure 1. A bar graph showing sexual dysfunction in males and females.
Gender Dysphoria and Transgender People
The behaviours, emotions, and attitudes a person’s culture connects with biological sex are defined as gender. Gender dysphoria refers to psychological distress caused by incongruence between an individual’s biological sex and gender identity. Transgender refers to individuals whose physical gender does not match their gender identity (Stangor and Walinga, 2010). Some transgender individuals may experience gender dysphoria. As a result, they may look for various areas of gender affirmation, like altering one’s name and pronouns or social affirmation. However, gender identity should not be mistaken for sexual orientation. The categories of persons that a person is sexually attracted to are referred to as their sexual orientation.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, provides a gender dysphoria diagnosis for children, adolescents, and adults using several criteria. At least two of the following are indicative of it in both adults and adolescents: A great desire for the sex traits of the other gender, a strong want to be of the other gender, a burning desire to be treated as the other gender, or a strong need to eliminate one’s primary or secondary sex denotation due to conflict with one’s expressed gender (Turban, 2022). A burning belief that one possesses the usual emotions and behaviours of the opposite gender is another.
Individuals suffering from gender dysphoria may alter their appearance, character, or interests. These individuals may show discomforts, such as low self-esteem, social withdrawal, depression and anxiety, and self-neglecting. In children, gender dysphoria may indicate the child’s interest in the other gender’s clothes or toys. A strong need to be the other gender, a significant dislike of an individual’s sexual anatomy, and a burning desire for cross-gender roles (Tarrant, 2022). Though this behaviour does not necessarily mean they have gender dysphoria, as it is common in childhood and part of growing up.
Transgender people suffer from discrimination leading to a negative self-image and stigmatization, which leads to an increased rate of other mental health issues. The suicide rate among transgender individuals is higher. Transgender children often fall victim to bullying and discrimination at school.
Individuals with gender dysphoria may be supported through open-ended exploration of their feelings of gender identity with a therapist. It usually aims at aiding the individual to feel free to explore their gender in a way that corresponds to their internal sense. This may include taking steps to change their body physically. Besides counselling, gender dysphoria treatment may involve hormones and gender reassignment surgery.
More extensive treatment involving gender-affirming hormone treatment and medical procedures may be done (Cherry, 2020). Treatment may also include body alterations that align the individual’s external appearance with their internal sense. Unfortunately, individuals who cannot take any of these steps may experience anxiety and depression. Psychotherapy may assist individuals in feeling at ease expressing their internal sense of gender. The treatment may be accomplished by teaching the individuals to practice self-acceptance, manage stress, build a support network and improve relationships.
In conclusion, the sexual disorder is experienced when an individual faces challenges related to their ability to feel pleasure and respond sexually. The four types of sexual dysfunction include desire disorders, characterized by a lack of sexual interest; arousal disorders, or orgasm disorders, indicated by a delay in or absence of orgasms; and pain disorders, identified by the presence of physical pain during sexual activity. The sexual disorders that affect males include premature ejaculation and erectile disorder. Women are particularly susceptible to illnesses like female orgasmic dysfunction. The contradiction between a person’s physical sex and the gender they identify with, on the other hand, is what leads to gender identity disorder. Gender identity disorder can be diagnosed in children, adolescents, and adults. In children, the child might prefer cross-dressing and want to be of the other sex. In adults and adolescents, it manifests through desperation to remove the primary and sexual characteristics. Therefore, it is important to emphasize that these disorders may be treated through therapy and medications.
References
Avasthi, A., Grover, S., & Rao, S. (2017). Clinical practice guidelines for management of sexual dysfunction. Indian Journal of Psychiatry, 59(1), 91-115. doi: 10.4103/0019-5545.196977
Cherry, K. (2020). What is Gender Dysphoria? Verywell Mind https://www.verywellmind.com/gender-dysphoria-5085081
Giorgi, A. (2020). What you need to know about dyspareunia (Painful intercourse). Healthline. https://www.healthline.com/health/dyspareunia
Reed, G. M., Drescher, J., Krueger, R. B., Atalla, E., Cochran, S. D., First, M. B., … & Saxena, S. (2016). Disorders related to sexuality and gender identity in the ICD‐11: Revising the ICD‐10 classification based on current scientific evidence, best clinical practices, and human rights considerations. World Psychiatry, 15(3), 205-221. https://doi.org/10.1002/wps.20354
Solis-Moreira, J. (2021). All about sexual dysfunction. PsychCentral. https://psychcentral.com/disorders/sex-overview#sex-addiction
Stangor, C., & Walinga, J. (2010). 13.6 Somatoform, Factitious, and Sexual Disorders. https://ecampusontario.pressbooks.pub/niagaracollegeintrotopsych/chapter/12-6-somatoform-factitious-and-sexual-disorders/
Tarrant, G. (2021). Gender identity disorder: Symptoms, causes, and treatments. PsychoTreat. https://psychotreat.com/gender-identity-disorder/
Turban, J. (2022). What is Gender Dysphoria? American Psychiatric Association. https://www.psychiatry.org/patients-families/gender-dysphoria/what-is-gender-dysphoria
 write
write