Introduction
Accessibility to healthcare has been a significant concern for decades. The increase in cases of patients’ inability to acquire treatment motivates researchers to explore the contributing factors. Researchers suggest that health disparities influence patients’ ability to obtain quality healthcare. Health disparities can be interpreted in various ways, such as one’s inability to access quality care due to racism, ethnicity, income, education, and other social determinants. Health disparities are associated with inferior health outcomes and increased mortality among minority groups. This analysis details the oral health disparities, the awareness of oral health, and the measures developed to address oral health disparities.
Oral health coverage is one of the most significant ways oral health disparities are still active through the health care system. Medicare is a federal program that provides health coverage to individuals over 65 or under 65 and has disabilities, no matter their income. On the other hand, Medicaid is a state and federal program that provides health coverage to individuals who have low income.
Medicaid and Medicare cover medical care to varying degrees and include a multitude of services; however, they fail to provide, if any coverage at all, when it comes to oral health care coverage. Many Americans cannot afford regular checkups, cleanings, and other dental procedures necessary for maintaining oral health. As a result of limited health insurance coverage, low-income and minority groups have poorer oral health than individuals of high socioeconomic statuses.
Medicare does not cover most dental services (including cleanings, fillings, tooth extractions, dentures, dental plates, or other dental devices). Medicare Part A (Hospital Insurance) covers some dental services received while in the hospital. Part A can pay for hospital stays if you need emergency or complex dental surgeries, even though it does not cover preventative dental care. Non-covered services, like most dental treatments, are entirely the patient’s responsibility (“Dental Services,” n.d.). Therefore, many people who participate with federally funded insurances decide to put off seeing a dentist until an emergency arises because they want to avoid the high expense of dentistry. This can result in an improper diagnosis and a more serious illness down the line. Medicaid has even worse plans since it completely excludes dental coverage in most states, leaving millions of people with little or no access to dental care.
Most people know that getting your teeth cleaned and examined by dental professionals every six months is vital to maintaining good oral health and hygiene. On the other hand, patients are often unaware that untreated dental caries might lead to other health problems. Untreated caries cause oral infections in the jaw bone, leading to conditions such as osteomyelitis or periodontitis, which are both inflammatory diseases of the bone around your teeth that are causing a great deal of pain and discomfort. Cardiovascular disease, diabetes, and premature birth in pregnant women are associated with untreated dental caries
Untreated dental caries can lead to further medical problems in children and adults. The first stage of dental caries is painless and often goes unnoticed. According to the Centers for Disease Control (CDC), untreated dental disease can cause pain and infection and lead to more severe issues like heart disease, diabetes, stroke, and premature birth.
Out of the many illnesses that can arise from untreated dental caries, one of the major issues is that it can lead to cardiovascular disease. Disease complexities occur when the bacterium that triggers periodontal disease inflames the gums, the germs can enter the circulation and cause plaque to build up and harden in the arteries. Atherosclerosis is the medical term for artery hardening, and it is a dangerous condition. It causes blood flow issues and cardiac obstructions and an increased risk of a heart attack. The damage to the arteries and blood vessels can cause hypertension and raise the risk of stroke. Endocarditis, which happens when the heart’s lining gets infected and is generally deadly, can also develop.
Increased insurance availability for children and Medicare seniors has made significant headway in this area of inequity. However, due to the highly political nature of the subject, no meaningful progress has been achieved in extending Medicaid coverage for low-income individuals. Low-income households sometimes lack the financial resources to take their entire family to the dentist.
The lack of coverage with oral health care is challenging to quantify because there are no national surveys on oral health status among adults and even less data on poor adults of different ethnic backgrounds due to small numbers within each ethnic group.
Some estimates do exist, though:
In 2015, 29 percent of Americans did not possess dental insurance, with 62 percent of elderly adults also falling into this category. Since standard Medicare does not provide primary dental care, many seniors lose this coverage after retiring. Furthermore, several low-income individuals lack access to governmental dental coverage. Adult Medicaid members are not obligated to receive dental services; hence dental coverage varies significantly from state to state. In total, there are 15 states that currently offer no coverage or just in case of emergencies. (“Disparities in Oral Health,” 2021).
The American Dental Association investigated dental benefits coverage in the U.S. In 2015, 10.3 percent of adolescents did not have coverage for any dental services, the lowest percentage ever, down from 15.8% in 2010. They also found that 38.5% of
children had dental coverage from Medicaid or CHIP (Children’s Health Insurance Program). CHIP is a Medicaid-affiliated program designed for children to receive health care. CHIP is a program that provides low-cost healthcare insurance to children whose families make more than is allowed amount for Medicaid recipients. CHIP does cover pregnant women in various states. Each state offers CHIP insurance and collaborates extensively with its Medicaid plans (“Dental coverage, barriers, and outcomes,” 2015).
Figure 1:
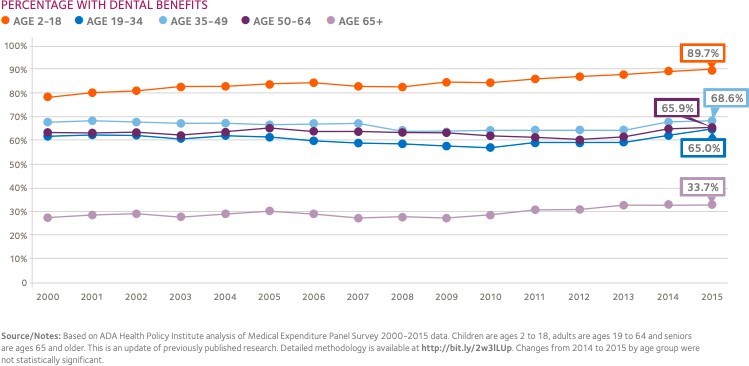
This figure shows that dental benefits decrease with an increase in age. Children between 2-18 years are the highest dental benefits at 89.7 percent, while individuals above 65 years have the lowest at 33.7 percent. Dental benefits for seniors are moderate and range between 65-70 percent. Children are prone to dental diseases; hence, many of them have dental health coverage. The rate of subscription of the seniors to dental health coverage is moderate as their prevalence of oral health diseases is average. On the other hand, dental benefits for the aged are the lowest as they are not educated on maintaining dental health.
Today, the importance of oral health is recognized. Oral health is an essential part of overall health, and oral health problems can affect our quality of life and our ability to function. Oral health is necessary for children, adults and the aged. Numerous measures have been enacted by the government, which include: the enactment of laws that prohibit discrimination in health care access; the creation of a new national body entitled the Office on Minority Health; and the development of programs designed to reduce health disparities. Throughout the years, many groups have been formed to raise awareness and effect change. One America Foundation, for example, was created in 2001 to bring together many parties to reduce health inequalities via education and advocacy in all parts of our communities, including institutions, churches, corporations, and medical centers.
Oral health inequalities have a variety of causes. In a lot of cases, socioeconomic reasons are to blame. In other circumstances, the absence of adequate services such as fluoridated water supply exacerbates these inequities. Some people might not have access to transportation to a facility or the freedom to take time off work to respond to their medical needs. Physical disabilities or other conditions may restrict access to care. Another obstacle is a lack of financial means to fund the care they need; whether they choose to pay out of pocket or through dental insurance, the cost of care remains high. Dental insurance is less common than medical insurance, and it is frequently forfeited when a person retires. As previously stated, public dental insurance plans are frequently subpar. A deficiency of public knowledge and education on the significance of oral health is another critical obstacle to seeking and receiving professional oral health treatment.
Measures and Interventions for Oral Health Disparities
The enactment of laws established on discrimination in health facilities can reduce oral health disparities. According to Patrick et al. (Pg 12), dentistry literature suggests that dentists have a negative attitude toward poor people as an oral health treatment is offered depending on the economic status of the patients. Besides, most public health facilities providing quality oral health services at a high cost discriminate against the poor as they cannot afford them. The enacted laws on oral health improve dentists’ perception of the minority’s practices and values and reduce the discriminatory activities of professional dentists. The current legislation for equality in health facilities can enhance the oral health of the poor by bridging the cultural gap and reducing the social perceptions on the economic status of patients. Preventing discrimination in health facilities by enacting laws reduces oral health disparities.
Public health program expansion is an appropriate counter to oral health disparities. According to Northridge et al.(Par 5), public oral health programs such as Medicare and Medicaid are essential as they offer affordable health services to promote the health of the poor. However, a large number of the poor in the society against the limited number of public health coverage programs reduces the accessibility to healthcare. Expansion of healthcare programs includes increasing dental healthcare teams and fluoridation plans. Healthcare programs’ expansion promotes oral health by their ability to reach the poor neighborhoods. Fluoridation expansion aims to prevent the accessibility of safe drinking water by using socioeconomic status and encouraging equality in the accessibility of treated water. Dental healthcare teams’ expansion measures involve employing more dental specialists to address oral health problems in public schools. Addressing oral health disparities in public schools is based on equality and can reduce congestion in dental healthcare facilities. Therefore, the expansion of fluoridation and health care teams reduces oral health disparities.
Community mobilization and collaboration efforts can prevent oral health disparities. Unequal allocation of healthcare services among communities and states is a critical contributing factor to the significant increase in oral health disparities (Patrick et al. Pg 14). Discrimination experienced in public health facilities in offering dental health services contributes to the increased cases of oral health problems among the poor. Community-organized programs and collaborative efforts can influence the government to increase the allocation of resources to improve community-based social facilities such as schools and hospitals. The establishment of zoning policies through community-based programs facilitates equality in offering investment opportunities that enhance the economic status of the poor. Community-based movements can induce the government to schedule oral health education programs among the poor in the society hence reducing cases of tooth decay for the minority. Community mobilization and collaboration promote the oral health of the poor by increasing economic status and facilitating health education.
Adoption of new technology in healthcare can reduce oral health disparities. According to Patrick et al. (Pg 14), the dental professional is the critical link between the oral health patients and the newly invented technology, determining the prevalence of oral diseases. Advancements in technology in healthcare promote the development of new treatment methods and medication at an affordable cost. Medication such as xylitol and fluoride varnish has been achieved by technological advancement and promoting quality and affordable treatment for dental caries and tooth decay. Further technology improvements can address oral health disparities resulting in effectiveness and equality in treating dental health infections. Dental health professionals advise the poor on the new and effective medication for oral health infections. Advancements in technology are essential in addressing oral health infections and disparities.
Improving funding for Medicaid health coverage for dentists and patients facilitates the improvement of oral health. According to Northridge et al.(Par 7), Medicaid is a federal health coverage program that aims to reimburse healthcare medical bills for the poor in society. The Medicaid program is associated with inefficient reimbursement systems, resulting in dentists’ rejection of patients and preventing access to quality medication for oral health diseases. The establishment of state-based policies on increasing Medicaid financing and enhancing Medicaid collaboration with professional associations can promote accessibility of oral health treatment by the poor. Besides this, Medicaid programs can achieve efficiency by revising the reimbursement systems, expanding dental treatment options, effectiveness in payment schedules, and encouraging dentists’ participation in Medicaid programs. The poor accessibility to quality healthcare can be achieved by proper management and efficiency of Medicaid programs. Improved financing of Medicaid programs is an appropriate solution to oral health disparities.
Promoting dental healthcare coverage can reduce oral health disparities. According to Patrick et al. (Pg 13), most communities perceive medical health coverage more essential than dental health coverage. In addition, the poor are unaware of the essence and importance of maintaining oral health as they misunderstand the importance of quality life. Various programs, such as the establishment of the office of minority health, facilitate the development of policies to address issues of oral health relating to the poor. Implementing community-based education programs effectively promotes awareness of oral health among the poor. The promotion of affordable Medicaid coverage programs and efficient reimbursement systems can enhance dental health coverage among the poor hence resulting in the accessibility of oral health services. Establishing oral health education programs, efficient reimbursement systems, and affordable coverage can address financial oral health disparities. The promotion of dental health coverage can therefore address oral health disparities.
Conclusion
Health disparities have a significant influence on the accessibility of healthcare services. Oral health disparities determine the quality and maintenance of oral health diseases. The rate of increase or decrease in oral health infections is influenced by the extent of awareness of the importance of maintaining the quality of life in society. Researchers suggest that discrimination based on race and ethnicity is associated with oral health disparities. Financial differences influence the affordability and the quality of oral health services hence the poor strain to maintain their dental health. Various methods such as improved financing for Medicaid programs, technology advancements, and community mobilizations have been developed counter oral health disparities and increase the accessibility of oral healthcare.
Works Cited
Centers for Disease Control and Prevention. (2020, December 2). Adult oral health. Centers for Disease Control and Prevention. Retrieved May 1, 2022, from https://www.cdc.gov/oralhealth/basics/adult-oral-health/index.html
Centers for Disease Control and Prevention. (2021, February 5). Disparities in Oral Health.
Centers for Disease Control and Prevention. Retrieved May 1, 2022, from https://www.cdc.gov/oralhealth/oral_health_disparities/index.htm
Dental coverage, barriers, and outcomes. Coverage, Access & Outcomes | American Dental Association. (2015). Retrieved May 2, 2022, from https://www.ada.org/resources/research/health-policy-institute/coverage-access-outcomes #:~:text=What%20share%20of%20U.S.%20children,do%20not%20have%20dental%20b enefits.
Dental Services. Dental service coverage. (n.d.). Retrieved May 1, 2022, from https://www.medicare.gov/coverage/dental-services
Healthy People 2010 : understanding and improving health. (2000). U.S. Dept. of Health and Human Services, Office Office of Public Health and Science, c 2000.
U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2000.
Northridge, Mary E. et al. “Disparities In Access To Oral Health Care.” Annual Review Of Public Health, vol 41, no. 1, 2020, pp. 513-535. Annual Reviews, https://doi.org/10.1146/annurev-publhealth-040119-094318. Accessed May 18, 2022.
Patrick, Donald L et al. “Reducing Oral Health Disparities: A Focus On Social And Cultural Determinants”. BMC Oral Health, vol 6, no. S1, 2006. Springer Science And Business Media LLC, https://doi.org/10.1186/1472-6831-6-s1-s4. Accessed May 18 2022.
 write
write