Introduction
The study was carried out with the aim of strategizing the most effective ways of reducing public mental health stigma among university students. The strategy was through a program made of psychoeducation and contact-based learning. Public stigma can be described as when the general public tends to endorse negative stereotypes and discrimination against individuals with mental illness (Gaebel et al., 2016); World Health Organization (2007). There is a more significant association between being mentally ill and negative characteristics like being a danger and violent to others (Schlier et al., 2016). Such beliefs tend to drive the whole community into fearing and avoiding these mentally ill individuals. This, however, is just a mere misconception about the individuals who have been determined to have mental issues. For instance, there is a widespread belief that individuals who have been diagnosed with schizophrenia tend to be very violent (Schlier et al., 2016). In general, shared and falsified beliefs have a significant impact on the perception of the whole community to exhibit a prejudicial and discriminatory emotional response and behavior.
A psychoeducation program, Mental Health First Aid (MHFA ), which was first developed and used in Australia in 2002, was repeated with the same intentions of improving the knowhow so as to offer assistance in the creation of a positive attitude and behavior on mental problems (Hadlaczky et al., 2014). The investigation measured the levels of knowledge the individual was able to retain, the changes, and the behavior. All the outcomes predicted were backed by the results found.
A study of the same type was aimed at providing education to high school teachers by (Jorm et al.,2010). The experiment had the foundational belief that high school teachers were better placed to provide much-needed assistance to learners who have been found to be developing mental health issues (Jorm et al. (2010). It was established that MHFA trainings were a success in the increase of psychoeducation, changing the beliefs on the treatment, aiding in the reduction of the stigma, and an increase in the confidence in giving help. Through the knowledge, the educators in Jorm’s research showed higher levels of confidence in being able to address the issues, thus making them more willing to provide help.
A research carried out by (Schlier et al.,2016) executed the use of three psychoeducation texts that focus on information on medications, cognitive behavioral Therapy (CBT), and psychotherapy. The study measured the impacts of the stereotype beliefs and the emotional response on schizophrenia. It was established that all three types of information on medication and treatment were more effective in the reduction of the stigma perceptions. Information on cognitive behavior therapy (CBT) was also very effective in the reduction of stigma as it reduced a substantial amount of pessimistic ideas the respondents had beforehand. All factors and conditions have indicated a reduction in the perceived dangers, unpredictability, incompetence, and anxieties towards individuals who have schizophrenia.
In this research, the aim is to investigate the effectiveness of the MBB2 clinical Psychology program on university students in reducing public stigma associated with mental health to reduce false and harmful stereotypes, prejudicial emotions, and segregated behavior. This MB2 program is also to address the same issues as highlighted by Jorm’s study (2010), aiming at educating so as to prevent false stereotypical beliefs and behavior directed towards mental illness. The study has hypothesized that the program will be a success in the reduction of harmful and misleading stereotypes based on the dangerous scale.
On the same note to Hadlaczky, this investigation also applied a scale for the assessment of the changed behavior in measuring stigma pre and post-BB2 program. Similarly, another hypothesis was formulated that hypothesized that the MBB2 clinical psychology program would be a success in the reduction of discriminatory behaviors in regard to mental illness as measured by the social distancing scale.
In the course of the MBB2 programmer, the psychoeducational and contact-based program was aimed at the provision of sufficient information so as to reduce anxiety and prejudicial emotions on mental health. This is similar to Schiller’s study on stereotypical beliefs and emotional responses to schizophrenia (2016). Based on the same principle, final predictions were produced for the hypothesis that the MBB2 clinical psychology program will be a success in the reduction of the prejudicial emotional responses in individuals with mental illness based on the Affective Reaction Scale.
METHOD
The method section is provided for.
RESULTS
For testing the hypothesis of the MBB2 program, the original scale applied for every hypothesis underwent modification so that all the findings lead to a positive direction. As the values of the scale rose, the figure was a representation of the reduced stigma. The means standard error of the scales was computed so as to gate the quantitative data. The comparison of the data was then put in a bar chart as shown below:
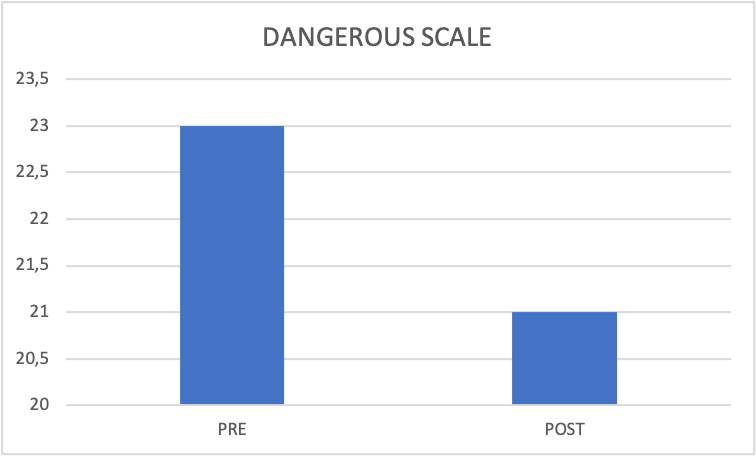
From the chart, the differences between the mean results pre and post-program were computed at lower significance than other scales, with a difference of 1.18. There were fewer standard errors with the pre-interventions at 0.18 and the post at 01.7. A one-tailed repeated measure t-test showed that the preprogram at M= 22.66 and SD=0.18 had higher significance in mean than the post at M=20.97 and SD= 0.17, with a t score of (770) =7.86, p<.05.
For the second hypothesis, it is shown in the chart below:
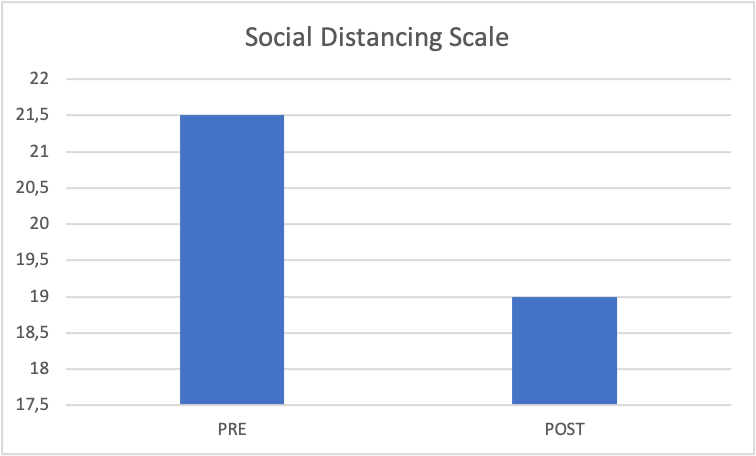
The mean formed indicated that the preprogram, M=21.5, SD=0.28, which was of higher significance than the post-MBB2 at M=19.0, SD=0.25, intervention. The one-tailed repeat measure of the test evidenced a significant difference in pre and post-effects of the psychoeducation program at t (771) =7.80, p<.05.
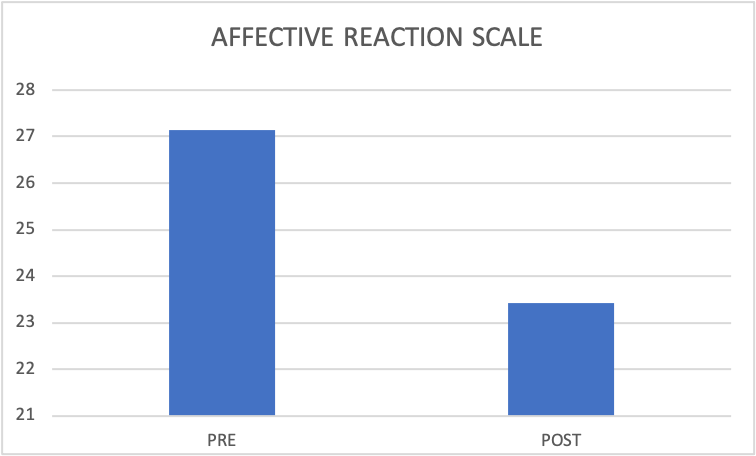
On the third hypothesis, the pre and post-MBB2 program findings indicated a reduction in the mean and SD Errors. The pre-intervention errors were 0.25, and the post was 0.22. The one-tailed repeat measure t-test showed a significant in the findings difference of the program for pre and post as t (771) =13.36, p<.05. This is an indication that the pre-MBB2, on average, has a high effective reaction score of M=27.15, SD=7.1 as compared to the post medication at M=23.42, SD=0.23/.
DISCUSSION
The experiment investigated the impact of the MBB2 clinical modules using a questionnaire on the basis of three scales. The hypothesis was that there would be fewer harmful stereotypes that can cause stigma as exhibited on mental illness after completing the MBB2 program, as shown by the dangerous scale. The mean of the post is higher than that of the post. In the second hypothesis, the social distancing scale after the modules was lower as compared to the pre-modules. In the last hypothesis, it was predicted that it would reduce the negative emotional response to mental illness, as shown by the affective reaction scale. The data collected was in support of the claims by the last hypothesis, with the mean pre-intervention being lower as compared to psychoeducational programming.
The dangerous scale had the lowest mean difference of the two conditions at a mean of 1.18, implying that it was the least effective. These harmful and misled stereotypes were less affected by modules in comparison to the high school educators (Jorm et al.,2010), which showed an increase in the knowledge of educators changed stereotypes on the treatment of mental illness to encourage them to assist students who have mental issues. However, the impacts were in smaller to medium range sizes, with the results that last six months post-intervention.
Findings from the hypothesis showed that discriminatory behavior was reduced in the MBB2 program, as indicated by the scores on the social distancing scale. The mean difference of the score of the post and pre-intervention indicates moderate in comparison to hypothesis 1. In a previous study done by Hadlaczky et al. (2014), the findings from the MBB2 program indicated consistency with improvement in attitude and behaviors on mental health problems. On the same note, the behaviors in the MBB2 hybrid program showed a reduction with moderate difference prior to and post-program.
The results from the affective reaction scale applied to the third hypothesis showed the greatest difference in the score of the pre and post-intervention of the hybrid program. The mean difference scores suggest that the measure was successful and effective in the reduction of mental illness stigma. In the research on schizophrenia (Schlier et al., 2016), it was established that psychoeducation was a success in the reduction of negative pre-existing stereotypes of psychosis. It showed a significant reduction in the perception of dangerousness and anxiety in individuals with schizophrenia. The MBB2 program and past studies are both shown to have a substantial stigma.
The limitations of the investigation included the MBB2 program needing a control group, thus being difficult to pinpoint the effects, which were on the basis of the program alone. To add on, individual differences, like educational background, could be skewed. The degree of every student could affect how the pre-existing knowledge has been retained. The MBB2 psychoeducational section is part of the program option to be viewed in class or online. In overcoming the imitations in future studies, a control group needs to be kept to strengthen the research group. To prevent any bias, deception could be used to hide the true aim; this will have to be debriefed at the end.
CONCLUSION
The results all support the three hypotheses formed. It established that the MBB2 program was more effective in the reduction of prejudicial emotional responses, as shown by the affective reaction scale, and less successful for harmful and misled stereotypes, as measured by the dangerousness scale. The dangerousness scale indicated the least change; it showed significance. In future studies, sample groups need to be filtered to ensure all genders and groups.
References
Gaebel, W., Rössler, W., & Sartorius, N. (2016). The Stigma of Mental Illness — End of The Story? Springer.
Hadlaczky, G., Hokby, S., Mkrtchian, A., Carli, V., Wasserman, D. (2014). Mental Health First is an effective public health intervention for improving knowledge, attitudes, and behavior: A meta-analysis, International Review of Psychiatry, 26(4), 467-475.
Jorm, A., Kitchener, B., Sawyer, M., Scales, H., Cvetkovski, S. (2010). Mental health first aid training for high school teachers: a cluster randomized trial, BMC Psychiatry, 10, 51–62.
Schlier, B., Lange, P., Wiese, S., Wirth, A., Lincoln, T. (2016). The effect of educational information about treatments for schizophrenia on stigmatizing perceptions, Journal of Behaviour Therapy and Experimental Psychiatry, 52, 11-16.
 write
write